
by Ambassador [ret] Jimmy Kolker
Editor’s note: After retiring from the Foreign Service in 2007, Ambassador Kolker spent four years at UNICEF before moving to the U.S. Department of Health and Human Services. As Assistant Secretary for Global Affairs there, he dealt with a number of international health concerns, including Ebola, Zika, and HIV/AIDS. This piece is adapted from his Virtual Presentation to an online DACOR audience on April 8, 2020.
While the Coronavirus outbreak and pandemic found nearly all countries unprepared, U.S. lapses in addressing major documented flaws in our preparedness contributed to breakdowns of international collaboration and solidarity as well as institutional conflicts and stress on our health system at home.
The Ebola Legacy
Much of the current U.S. Government structure to deal with global outbreaks and epidemics was reviewed and developed based on the strengths and weaknesses of how we dealt with Ebola 2014-15. Thus, it is worth starting with the lessons of that experience.
The initial response of the global community, especially the World Health Organization, to the West Africa Ebola epidemic was late, ineffective and uncoordinated. U.S. leadership in bringing attention to the scope of the problem and mobilizing international response to Liberia, Guinea and Sierra Leone was indispensable. Field trials of U.S.-developed and other candidate vaccines and therapies were begun, but after the epidemic passed its peak and were not coordinated.
Likewise, the United States scaled up domestic preparedness, but hospital and health system readiness was never tested, as only three individuals whose infections were not first identified abroad presented for treatment in the U.S. Internal debate about Ebola policies never became highly partisan, nor was there a shortage of protective gear, diagnostics or hospital supplies.
In West Africa, the U.S. Agency for International Development foreign disaster assistance structure, along with surge capacity from the U.S. Centers for Disease Control and Prevention and the U.S. Public Health Service, ultimately rose to meet Liberia’s needs for Ebola treatment centers. The U.S. military provided timely but limited logistical support.
Although Blue Ribbon commissions set up to review the Ebola response and suggest measures for improvement found serious gaps, they unanimously concluded that there was no multilateral alternative to the World Health Organization in outbreak-led emergencies. (https://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1002042) Existing instruments already in place, such as the International Health Regulations (https://www.who.int/ihr/publications/9789241580496/en/) and the U.S.-initiated Global Health Security Agenda (https://ghsagenda.org/), should remain the foundation for an improved global response capacity.
With domestic systems not tested or found wanting, while the WHO implemented many of the recommended reforms and U.S. international engagement was judged largely positive, the Ebola experience did not engender major review or reinforcement of U.S. structures or level of effort. Emergency funds appropriated for the Ebola emergency ran out without being re-appropriated. We were left with a complacency that capacity would be sufficient to deal with an outbreak or epidemic.
Relations with China
The Severe Acute Respiratory Syndrome (SARS) outbreak that originated in the People’s Republic of China in 2003 revealed numerous lapses in both the Chinese ability to respond to and share information about the novel disease and the norms for international collaboration in the event of such an epidemic.

The Chinese government tried to address these shortcomings, notably by establishing a Chinese Center for Disease Control and Prevention (http://www.chinacdc.cn/en/), consciously modeled on the U.S. CDC. American CDC personnel assigned to China had their office within the Chinese CDC; in 2013, when Chinese epidemiologists identified a potentially severe outbreak of H7N9 avian influenza, CDC surged 40 additional staff to China to bolster Chinese surveillance and detection activities. U.S. and Chinese disease response teams worked together in Liberia during the 2014-15 Ebola outbreak. And the two nations collaborated with the African Union, as the leading foreign partners for the African CDC, (https://africacdc.org/about-us/) which was established in 2016.
The Trump Administration, however, called into question Chinese intentions and the value to the U.S. of health collaboration. The U.S. Department of Health and Human Services, which has personnel from the Food and Drug Administration (FDA) and the National Institutes of Health (NIH) as well as CDC based in China, was told to reduce its “footprint.” The process, begun in the Obama Administration, to bring all U.S. government employees posted abroad into U.S. government-controlled facilities for security reasons was accelerated, and most CDC staff moved from the China CDC to the embassy compound.
The total number of CDC employees (American and Chinese) in China fell from 47 in 2016 to 14. The last American CDC expert located on the China CDC campus, working directly to train Chinese epidemiologists through the Field Epidemiology Training Program, was brought home in July 2019.
When non-emergency personnel were evacuated from the U.S. embassy in Beijing in February 2020, all FDA and NIH staff were relocated to the United States. (https://www.wsj.com/articles/u-s-drawdown-of-china-diplomats-cripples-ties-at-critical-moment-11584788401)
This drastic reduction in historic levels of American government health experts interacting directly with Chinese counterparts is at least part of the reason that data and analysis of the SARS2 Coronavirus situation in China reaching the U.S. government was less complete and less timely than it should have been. Furthermore, the deteriorating quality and quantity of bilateral health relations likely contributed to Chinese refusals of U.S. offers of expert help and attempts to bring in additional specialists. (https://www.washingtonpost.com/politics/2020/04/03/how-much-pressure-did-trump-put-china-access-concerning-coronavirus/)
The National Security Council and the Interagency Process
The first staff specifically devoted to health security working for the White House National Security Council were in the Clinton Administration. President Barack Obama’s Directorate for Global Health Security and Biodefense, a 2016 post-Ebola formalization of NSC functions, was initially carried over into the Trump Administration, with four very strong professional staff and a clear executive order mandate (https://obamawhitehouse.archives.gov/the-press-office/2016/11/04/executive-order-advancing-global-health-security-agenda-achieve-world).
The Senior Director, Adm. Tim Ziemer, reported to NSC Homeland Security Advisor Tom Bossert. In 2018, in his first days as National Security Advisor, John Bolton abolished the jobs of both Bossert and Ziemer and dismissed them. (https://www.washingtonpost.com/news/to-your-health/wp/2018/05/10/top-white-house-official-in-charge-of-pandemic-response-exits-abruptly/) The reason given was streamlining the NSC staff around a small number of “hard” security issues; two of the former health security experts were moved to the division charged with counteracting weapons of mass destruction.
In that capacity, they completed two useful strategies, the National Biodefense Strategy (https://www.whitehouse.gov/wp-content/uploads/2018/09/National-Biodefense-Strategy.pdf) and the National Health Security Strategy (https://www.whitehouse.gov/wp-content/uploads/2019/05/GHSS.pdf).
These strategies set out that, in the event of a health security threat, a Task Force chaired by the Secretary of Health and Human Services (HHS), would lead the government response. The HHS assistant secretary for preparedness and response (ASPR) would coordinate the task force activities. And as first news of the coronavirus in Wuhan, China spread, HHS Secretary Alex Azar and ASPR Robert Kadlec activated the task force.
The limitations of this arrangement quickly became evident. HHS is a huge, but intensely domestic agency. HHS has little convening authority. The Department and its leadership have no mandate to lead on issues with broad security, economic, and foreign policy impact. Relations with the White House, including the acting Chief of Staff, who also headed the Office of Management and Budget, were frosty. (https://www.nytimes.com/2020/03/16/us/politics/kushner-trump-coronavirus.html)
From my own experience as the first Foreign Service officer to have a senior position at HHS, I know that HHS leadership has little knowledge of the workings of State, DOD, or USAID, and the latter two were not even members of the task force. Significantly, HHS has no ability to instruct U.S. embassies abroad, a key tool in trying to build international cooperation and find out where and how an epidemic is spreading.
In addition to diverting the inter-agency convening authority to a cabinet department that could not effectively exercise it, the elimination of the NSC health security and biodefense directorate reduced or marginalized two valuable functions. While CDC and others track outbreaks and disease threats around the world, the absence of a “smoke alarm” in the White House, with the responsibility to get the attention of political leadership and multi-agency expertise was likely costly. (https://www.washingtonpost.com/outlook/nsc-pandemic-office-trump-closed/2020/03/13/a70de09c-6491-11ea-acca-80c22bbee96f_story.html)
The White House is also the operational lead for preparing top-level meetings of the G7, comprising the world’s major economies, which in the post-Ebola period took a strong pro-active role in promoting WHO reform and worldwide preparedness. Reducing the status and staffing on health security likely contributed to the failure of the G7 to unite and push for concerted action on COVID-19. (https://www.cbc.ca/news/politics/g7-covid-19-coronavirus-wuhan-pompeo-trump-1.5510329).
The HHS-led task force was replaced in March by one led by the Vice President. The HHS Secretary, ASPR and CDC Director were sidelined, at least to the extent that they were not always at task force meetings or subsequent press briefings. (https://www.politico.com/news/2020/03/05/white-house-alex-azar-coronavirus-122250) (https://www.washingtonpost.com/health/2020/03/19/cdc-top-us-public-health-agency-is-sidelined-during-coronavirus-pandemic/) The health expert role was assumed by Drs. Anthony Fauci and Deborah Birx, both gifted scientists and communicators. It is my belief, however, that a number of tasks were neglected or performed clumsily because HHS leaders were not fully trusted or engaged. These include development and approval of an authoritative diagnostic test, and replenishment of the national stockpile for personal protective equipment (PPE) and hospital supplies, such as ventilators.
Internationally, the gaps were also apparent, with State and HHS/CDC under-performing and lacking visibility, including: no clear policy on import and export of PPE and essential supplies and drugs; disconnects with the WHO and their work in China; slow and underfunded efforts where the U.S. normally plays a leadership role in aiding disease response in Africa and Latin America; gross neglect of migrants and populations at risk in humanitarian emergencies.
“Nobody Saw This Coming”
The mind-set most Americans, including some of our political leadership, had toward a pandemic which could cause major disruption to the United States and our way of life might be compared to an asteroid. Yes, there is a risk that this low probability, high-consequence event could occur, and, yes, we should pay some experts to keep track of the threat. But there is no reason to factor the risk into our daily lives and no reason to spend money that could be used for more immediate needs on preparations or contingencies.
The much more relevant comparison should have been terrorism. In recent years, there have been frequent terrorist events, but since 2001, the U.S. has not been hit hard. 95% of the victims of terrorism in 2017 were in the Mideast, Africa and South Asia, and their numbers were in the tens of thousands, not millions. Nonetheless, 42% of Americans said they are worried or very worried about themselves or a family member being victim of a terrorist attack. (Our World in Data, 2019). The U.S. government spends hundreds of billions of dollars a year gathering intelligence, working with countries where terrorism is most likely to arise to minimize it, and preparing states, airports, cities and communities to prevent and combat terrorism.
Disease outbreaks with pandemic potential are eerily similar. There are dozens of them per year. Few have done major damage in the United States, and the death tolls have been in the tens of thousands. But even as experts predicted the probability of a devastating epidemic, on a par with the 1918 Spanish flu that killed 675,000 Americans (https://www.history.com/topics/world-war-i/1918-flu-pandemic), U.S. government efforts to prevent, predict, prepare for and combat global outbreaks and epidemics were a tiny fraction of what we are spending on combatting terrorism.
There were numerous warning documents and analyses, easily available to the Administration. The Obama administration left a Playbook for Early Response to High Consequence Infectious Disease Threats. (https://www.politico.com/news/2020/03/25/trump-coronavirus-national-security-council-149285) More recently, the Center for Strategic and International Studies organized a commission on health security, which issued a report in December 2019, Ending the Cycle of Crisis and Complacency in U.S. Global Health Security. (https://www.csis.org/analysis/ending-cycle-crisis-and-complacency-us-global-health-security) (Disclosure: I contributed to the Playbook and was a member of the CSIS commission).
Bottom Line: Lots of people saw this coming and made their concerns vocal and repeated.
“But the U.S. is the Best Prepared Country in the World”
Yes, the Global Health Security Index (https://www.ghsindex.org/) put out in 2019 by the Nuclear Threat Initiative and Johns Hopkins University Center for Health Security, graded the United States 83.5 out of a possible 100 based on 34 indicators of preparedness for a major disease outbreak, the highest of all 195 countries.
However, if we look at the individual indicators more closely, the U.S. scored only 60% on “Health capacity in clinics, hospitals, and community care centers.” The score was even lower, 25%, on “Healthcare access” and the United States scored zero, repeat, zero, on “Exercising Response Plans.”
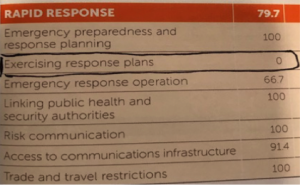
We are seeing vividly the consequences of mediocre preparedness of hospitals and clinics, the inequalities and lapses in access to care, and the failure to exercise our readiness plans and put a team in place ready to meet the challenge of Coronavirus. One lesson from our late-starting and uncoordinated response to the Ebola outbreak is that exercising our preparations and response forces is essential. It is an activity the federal government can best lead, as it does on military exercises.
Bottom Line: The U.S. was well-prepared compared to others, but we did not address major documented flaws in our preparedness and these are exactly the areas where the response has broken down.
Where is the State Department?
As diplomats, we recognize the pivotal role that the State Department and U.S. missions abroad play in any global emergency. However, State has been notably absent at all levels in the U.S. actions to combat COVID-19.
The office responsible for outbreaks is OES/IHB, the Office of International Health and Biodefense in the Bureau of Oceans, Environment and International Scientific Affairs. This is the only State Department bureau for which the Trump Administration has never even nominated an Assistant Secretary. The bureau and the IHB office are staffed largely by civil servants, and the Environment, Science, Technology and Health (ESTH) officers, serving in U.S. embassies overseas, are almost never health experts. In my experience and observation, OES/IHB is challenged to get the attention of State’s embassies and geographic regional bureaus, who are central to bilateral relations, and even less able to influence decisions of the seventh floor, where the Department leadership sits. That seems to be true for COVID-19 as well.
Secretary Hillary Clinton in 2012 established an Office of Global Health Diplomacy (GHD), independent of OES and to be headed by an ambassador. The only people named to head the office, however, have been the U.S. Global AIDS Coordinators. Although each has been a prominent health professional holding the title of ambassador, these coordinators have even less day-to-day contact than OES with State’s geographic bureaus, Department principals, or embassies abroad except on AIDS matters. The small GHD staff is located in the AIDS Coordinator’s office, a mile away from State Department headquarters.
The State Department’s preoccupation has been the health and repatriation of U.S. citizens, including USG employees and their families around the world, not with big-picture global action to combat the pandemic. Thus, the United States is missing opportunities to exert the leadership we customarily have done with multilateral organizations (WHO, World Bank, UN Security Council, G7, G20), areas of traditional U.S. development partnership (Latin America and the Caribbean, Africa, conflict and humanitarian situations) and reduced information gathering, policy influencing, and compassionate engagement everywhere.
What Are Some Consequences?
There is and will be continuing competition, rather than a good-faith effort at collaboration in the development of countermeasures – therapies, vaccines – and sharing needed supplies.
The resulting zero-sum problems of intellectual property, sovereignty, and ability to commandeer valuable products in short supply for national use will be more intense than the health community has ever seen.
As we see, low-and-middle-income countries, already underserved, have difficulty acquiring and deploying diagnostic tests, PPE and hospital supplies. Supply chains are disrupted and existing arrangements are frequently short-circuited by force majeure.
Issues of equity will be more important, but also more challenging than ever, once therapies and vaccines are approved for use. There is no mechanism to determine greatest need, and both the U.S. and China have energetically tried to meet domestic needs ahead of any international obligations.
As China’s health situation improves, however, Beijing, and Chinese institutions have already shown that they will try to make a splash by offering supplies and, eventually, countermeasures, to needy partners, rich and poor. There is a vacuum of global health leadership, a role played by the United States for nearly a century. China appears more ready than any other stakeholder to fill it. The deficit in leadership means that we have yet to see the global cooperation required to address the pandemic. The U.S. can and should see health diplomacy as a means to demonstrate the global leadership our dire situation calls for.![]()
 Ambassador Jimmy Kolker is a visiting scholar at Georgetown University’s Center for Global Health Science and Security and a fellow at the Center for Strategic and International Studies. During a 30-year career with the Department of State, he served as ambassador to Burkina Faso and Uganda. After retiring from the foreign service, he was Chief of the HIV/AIDS Section at UNICEF’s New York headquarters. From 2011-2017, as Assistant Secretary for Global Affairs at the U.S. Department of Health and Human Services (HHS), Amb Kolker represented the United States at World Health Organization meetings and as alternate Board Member of the Global Fund to Fight AIDS, Tuberculosis and Malaria.
Ambassador Jimmy Kolker is a visiting scholar at Georgetown University’s Center for Global Health Science and Security and a fellow at the Center for Strategic and International Studies. During a 30-year career with the Department of State, he served as ambassador to Burkina Faso and Uganda. After retiring from the foreign service, he was Chief of the HIV/AIDS Section at UNICEF’s New York headquarters. From 2011-2017, as Assistant Secretary for Global Affairs at the U.S. Department of Health and Human Services (HHS), Amb Kolker represented the United States at World Health Organization meetings and as alternate Board Member of the Global Fund to Fight AIDS, Tuberculosis and Malaria.